Chapter 12: Psychosocial Development in Infancy & Toddlerhood
Chapter 12 Learning Objectives
- Identify styles of temperament and explore goodness-of-fit
- Describe the infant emotions, self-awareness, stranger wariness, and separation anxiety
- Describe the early theories of attachment
- Contrast styles of attachment according to the Strange Situation Technique
- Explain the factors that influence attachment
- Use Erikson’s theory to characterize psychosocial development during infancy
Temperament
Perhaps you have spent time with a number of infants. How were they alike? How did they differ? How do you compare with your siblings or other children you have known well? You may have noticed that some seemed to be in a better mood than others and that some were more sensitive to noise or more easily distracted than others. These differences may be attributed to temperament. Temperament is the innate characteristics of the infant, including mood, activity level, and emotional reactivity, noticeable soon after birth.
In a 1956 landmark study, Chess and Thomas (1996) evaluated 141 children’s temperament based on parental interviews. Referred to as the New York Longitudinal Study, infants were assessed on 9 dimensions of temperament including: Activity level, rhythmicity (regularity of biological functions), approach/withdrawal (how children deal with new things), adaptability to situations, intensity of reactions, threshold of responsiveness (how intense a stimulus has to be for the child to react), quality of mood, distractibility, attention span, and persistence. Based on the infants’ behavioral profiles, they were categorized into three general types of temperament:
- Easy Child (40%) who is able to quickly adapt to routine and new situations, remains calm, is easy to soothe, and usually is in a positive mood.
- Difficult Child (10%) who reacts negatively to new situations, has trouble adapting to routine, is usually negative in mood, and cries frequently.
- Slow-to-Warm-Up Child (15%) has a low activity level, adjusts slowly to new situations and is often negative in mood.
As can be seen the percentages do not equal 100% as some children were not able to be placed neatly into one of the categories. Think about how you might approach each type of child in order to improve your interactions with them. An easy child will not need much extra attention, while a slow to warm up child may need to be given advance warning if new people or situations are going to be introduced. A difficult child may need to be given extra time to burn off their energy. A caregiver’s ability to work well and accurately read the child will enjoy a goodness-of-fit, meaning their styles match and communication and interaction can flow. Parents who recognize each child’s temperament and accept it, will nurture more effective interactions with the child and encourage more adaptive functioning. For example, an adventurous child whose parents regularly take her outside on hikes would provide a good “fit” to her temperament.
Parenting is bidirectional: Not only do parents affect their children, children influence their parents. Child characteristics, such as temperament, affect parenting behaviors and roles. For example, an infant with an easy temperament may enable parents to feel more effective, as they are easily able to soothe the child and elicit smiling and cooing. On the other hand, a cranky or fussy infant elicits fewer positive reactions from his or her parents and may result in parents feeling less effective in the parenting role (Eisenberg et al., 2008). Over time, parents of more difficult children may become more punitive and less patient with their children (Clark, Kochanska, & Ready, 2000; Eisenberg et al., 1999; Kiff, Lengua, & Zalewski, 2011). Parents who have a fussy, difficult child are less satisfied with their marriages and have greater challenges in balancing work and family roles (Hyde, Else-Quest, & Goldsmith, 2004). Thus, child temperament is one of the child characteristics that influence how parents behave with their children.

Temperament does not change dramatically as we grow up, but we may learn how to work around and manage our temperamental qualities. Temperament may be one of the things about us that stays the same throughout development. In contrast, personality, defined as an individual’s consistent pattern of feeling, thinking, and behaving, is the result of the continuous interplay between biological disposition and experience.
Personality also develops from temperament in other ways (Thompson, Winer, & Goodvin, 2010). As children mature biologically, temperamental characteristics emerge and change over time. A newborn is not capable of much self-control, but as brain-based capacities for self- control advance, temperamental changes in self-regulation become more apparent. For example, a newborn who cries frequently does not necessarily have a grumpy personality; over time, with sufficient parental support and an increased sense of security, the child might be less likely to cry.
In addition, personality is made up of many other features besides temperament. Children’s developing self-concept, their motivations to achieve or to socialize, their values and goals, their coping styles, their sense of responsibility and conscientiousness, and many other qualities are encompassed into personality. These qualities are influenced by biological dispositions, but even more by the child’s experiences with others, particularly in close relationships, that guide the growth of individual characteristics. Indeed, personality development begins with the biological foundations of temperament but becomes increasingly elaborated, extended, and refined over time. The newborn that parents gazed upon becomes an adult with a personality of depth and nuance.
Infant Emotions
At birth, infants exhibit two emotional responses: Attraction and withdrawal. They show attraction to pleasant situations that bring comfort, stimulation, and pleasure, and they withdraw from unpleasant stimulation such as bitter flavors or physical discomfort. At around two months, infants exhibit social engagement in the form of social smiling as they respond with smiles to those who engage their positive attention (Lavelli & Fogel, 2005).

Social smiling becomes more stable and organized as infants learn to use their smiles to engage their parents in interactions. Pleasure is expressed as laughter at 3 to 5 months of age, and displeasure becomes more specific as fear, sadness, or anger between ages 6 and 8 months. Anger is often the reaction to being prevented from obtaining a goal, such as a toy being removed (Braungart-Rieker, Hill-Soderlund, & Karrass, 2010). In contrast, sadness is typically the response when infants are deprived of a caregiver (Papousek, 2007). Fear is often associated with the presence of a stranger, known as stranger wariness, or the departure of significant others known as separation anxiety. Both appear sometime between 6 and 15 months after object permanence has been acquired. Further, there is some indication that infants may experience jealousy as young as 6 months of age (Hart & Carrington, 2002).
Emotions are often divided into two general categories: Basic emotions, such as interest, happiness, anger, fear, surprise, sadness and disgust, which appear first, and self-conscious emotions, such as envy, pride, shame, guilt, doubt, and embarrassment. Unlike primary emotions, secondary emotions appear as children start to develop a self-concept and require social instruction on when to feel such emotions. The situations in which children learn self- conscious emotions vary from culture to culture. Individualistic cultures teach us to feel pride in personal accomplishments, while in more collective cultures children are taught to not call attention to themselves unless you wish to feel embarrassed for doing so (Akimoto & Sanbinmatsu, 1999).
Facial expressions of emotion are important regulators of social interaction. In the developmental literature, this has been investigated under the concept of social referencing; that is, the process whereby infants seek out information from others to clarify a situation and then use that information to act (Klinnert, Campos, & Sorce, 1983). To date, the strongest demonstration of social referencing comes from work on the visual cliff. In the first study to investigate this concept, Sorce, Emde, Campos, and Klinnert (1985) placed mothers on the far end of the “cliff” from the infant. Mothers first smiled to the infants and placed a toy on top of the safety glass to attract them; infants invariably began crawling to their mothers. When the infants were in the center of the table, however, the mother then posed an expression of fear, sadness, anger, interest, or joy. The results were clearly different for the different faces; no infant crossed the table when the mother showed fear; only 6% did when the mother posed anger, 33% crossed when the mother posed sadness, and approximately 75% of the infants crossed when the mother posed joy or interest.
Other studies provide similar support for facial expressions as regulators of social interaction. Experimenters posed facial expressions of neutral, anger, or disgust toward babies as they moved toward an object and measured the amount of inhibition the babies showed in touching the object (Bradshaw, 1986). The results for 10- and 15-month olds were the same: Anger produced the greatest inhibition, followed by disgust, with neutral the least. This study was later replicated using joy and disgust expressions, altering the method so that the infants were not allowed to touch the toy (compared with a distractor object) until one hour after exposure to the expression (Hertenstein & Campos, 2004). At 14 months of age, significantly more infants touched the toy when they saw joyful expressions, but fewer touched the toy when the infants saw disgust.
A final emotional change is in self-regulation. Emotional self-regulation refers to strategies we use to control our emotional states so that we can attain goals (Thompson & Goodvin, 2007).
This requires effortful control of emotions and initially requires assistance from caregivers (Rothbart, Posner, & Kieras, 2006). Young infants have very limited capacity to adjust their emotional states and depend on their caregivers to help soothe themselves. Caregivers can offer distractions to redirect the infant’s attention and comfort to reduce the emotional distress. As areas of the infant’s prefrontal cortex continue to develop, infants can tolerate more stimulation. By 4 to 6 months, babies can begin to shift their attention away from upsetting stimuli (Rothbart et al, 2006). Older infants and toddlers can more effectively communicate their need for help and can crawl or walk toward or away from various situations (Cole, Armstrong, & Pemberton, 2010). This aids in their ability to self-regulate. Temperament also plays a role in children’s ability to control their emotional states, and individual differences have been noted in the emotional self-regulation of infants and toddlers (Rothbart & Bates, 2006).
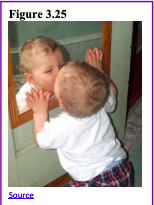
Development of sense of self: During the second year of life, children begin to recognize themselves as they gain a sense of self as object. In a classic experiment by Lewis and Brooks (1978) children 9 to 24 months of age were placed in front of a mirror after a spot of rouge was placed on their nose as their mothers pretended to wipe something off the child’s face. If the child reacted by touching his or her own nose rather that of the “baby” in the mirror, it was taken to suggest that the child recognized the reflection as him- or herself. Lewis and Brooks found that somewhere between 15 and 24 months most infants developed a sense of self-awareness. Self-awareness is the realization that you are separate from others (Kopp, 2011).
Once a child has achieved self-awareness, the child is moving toward understanding social emotions such as guilt, shame or embarrassment, as well as, sympathy or empathy.
Forming Attachments
Attachment is the close bond with a caregiver from which the infant derives a sense of security. The formation of attachments in infancy has been the subject of considerable research as attachments have been viewed as foundations for future relationships. Additionally, attachments form the basis for confidence and curiosity as toddlers, and as important influences on self-concept.

Freud’s Psychoanalytic Theory: According to Freud (1938) infants are oral creatures who obtain pleasure from sucking and mouthing objects. Freud believed the infant will become attached to a person or object that provides this pleasure. Consequently, infants were believed to become attached to their mother because she was the one who satisfied their oral needs and provided pleasure. Freud further believed that the infants will become attached to their mothers “if the mother is relaxed and generous in her feeding practices, thereby allowing the child a lot of oral pleasure,” (Shaffer, 1985, p. 435). Was Freud correct in his explanation for why infants became attached?
Harlow’s Research: In one classic study showing if nursing was the most important factor to attachment, Wisconsin University psychologists Harry and Margaret Harlow investigated the responses of young monkeys. The infants were separated from their biological mothers, and two surrogate mothers were introduced to their cages. One, the wire mother, consisted of a round wooden head, a mesh of cold metal wires, and a bottle of milk from which the baby monkey could drink. The second mother was a foam-rubber form wrapped in a heated terry-cloth blanket. The infant monkeys went to the wire mother for food, but they overwhelmingly preferred and spent significantly more time with the warm terry-cloth mother. The warm terry-cloth mother provided no food but did provide comfort (Harlow, 1958). The infant’s need for physical closeness and touching is referred to as contact comfort. Contact comfort is believed to be the foundation for attachment. The Harlows’ studies confirmed that babies have social as well as physical needs. Both monkeys and human babies need a secure base that allows them to feel safe. From this base, they can gain the confidence they need to venture out and explore their worlds.
Bowlby’s Theory: Building on the work of Harlow and others, John Bowlby developed the concept of attachment theory. He defined attachment as the affectional bond or tie that an infant forms with the mother (Bowlby, 1969). An infant must form this bond with a primary caregiver in order to have normal social and emotional development. In addition, Bowlby proposed that this attachment bond is very powerful and continues throughout life. He used the concept of a secure base to define a healthy attachment between parent and child (Bowlby, 1982). A secure base is a parental presence that gives the child a sense of safety as the child explores the surroundings.
Bowlby said that two things are needed for a healthy attachment: The caregiver must be responsive to the child’s physical, social, and emotional needs; and the caregiver and child must engage in mutually enjoyable interactions (Bowlby, 1969). Additionally, Bowlby observed that infants would go to extraordinary lengths to prevent separation from their parents, such as crying, refusing to be comforted, and waiting for the caregiver to return. He observed that these same expressions were common to many other mammals, and consequently argued that these negative responses to separation serve an evolutionary function.
Because mammalian infants cannot feed or protect themselves, they are dependent upon the care and protection of adults for survival. Thus, those infants who were able to maintain proximity to an attachment figure we’re more likely to survive and reproduce.
Erikson: Trust vs. Mistrust
As previously discussed in chapter 1, Erikson formulated an eight stage theory of psychosocial development. Erikson was in agreement on the importance of a secure base, arguing that the most important goal of infancy was the development of a basic sense of trust in one’s caregivers. Consequently, the first stage, trust vs. mistrust, highlights the importance of attachment. Erikson maintained that the first year to year and a half of life involves the establishment of a sense of trust (Erikson, 1982). Infants are dependent and must rely on others to meet their basic physical needs as well as their needs for stimulation and comfort. A caregiver who consistently meets these needs instills a sense of trust or the belief that the world is a trustworthy place. The caregiver should not worry about over indulging a child’s need for comfort, contact or stimulation.
Problems establishing trust: Erikson (1982) believed that mistrust could contaminate all aspects of one’s life and deprive the individual of love and fellowship with others. Consider the implications for establishing trust if a caregiver is unavailable or is upset and ill-prepared to care for a child. Or if a child is born prematurely, is unwanted, or has physical problems that make him or her less desirable to a parent. Under these circumstances, we cannot assume that the parent is going to provide the child with a feeling of trust.
Mary Ainsworth and the Strange Situation Technique
Developmental psychologist Mary Ainsworth, a student of John Bowlby, continued studying the development of attachment in infants. Ainsworth and her colleagues created a laboratory test that measured an infant’s attachment to his or her parent. The test is called The Strange Situation Technique because it is conducted in a context that is unfamiliar to the child and therefore likely to heighten the child’s need for his or her parent (Ainsworth, 1979).
During the procedure, that lasts about 20 minutes, the parent and the infant are first left alone, while the infant explores the room full of toys. Then a strange adult enters the room and talks for a minute to the parent, after which the parent leaves the room. The stranger stays with the infant for a few minutes, and then the parent again enters, and the stranger leaves the room. During the entire session, a video camera records the child’s behaviors, which are later coded by trained coders. The investigators were especially interested in how the child responded to the caregiver leaving and returning to the room, referred to as the “reunion.” On the basis of their behaviors, the children are categorized into one of four groups where each group reflects a different kind of attachment relationship with the caregiver. One style is secure and the other three styles are referred to as insecure.
- A child with a secure attachment style usually explores freely while the caregiver is present and may engage with the stranger. The child will typically play with the toys and bring one to the caregiver to show and describe from time to time. The child may be upset when the caregiver departs but is also happy to see the caregiver return.
- A child with an ambivalent (sometimes called resistant) attachment style is wary about the situation in general, particularly the stranger, and stays close or even clings to the caregiver rather than exploring the toys. When the caregiver leaves, the child is extremely distressed and is ambivalent when the caregiver returns. The child may rush to the caregiver, but then fails to be comforted when picked up. The child may still be angry and even resist attempts to be soothed.
- A child with an avoidant attachment style will avoid or ignore the mother, showing little emotion when the mother departs or returns. The child may run away from the mother when she approaches. The child will not explore very much, regardless of who is there, and the stranger will not be treated much differently from the mother.
- A child with a disorganized/disoriented attachment style seems to have an inconsistent way of coping with the stress of the strange situation. The child may cry during the separation, but avoid the mother when she returns, or the child may approach the mother but then freeze or fall to the floor.
How common are the attachment styles among children in the United States? It is estimated that about 65 percent of children in the United States are securely attached. Twenty percent exhibit avoidant styles and 10 to 15 percent are ambivalent. Another 5 to 10 percent may be characterized as disorganized (Ainsworth, Blehar, Waters, & Wall, 1978).
Some cultural differences in attachment styles have been found (Rothbaum, Weisz, Pott, Miyake, & Morelli, 2010). For example, German parents value independence and Japanese mothers are typically by their children’s sides. As a result, the rate of insecure-avoidant attachments is higher in Germany and insecure-resistant attachments are higher in Japan. These differences reflect cultural variation rather than true insecurity, however (van Ijzendoorn and Sagi, 1999). Overall, secure attachment is the most common type of attachment seen in every culture studied thus far (Thompson, 2006).

Caregiver Interactions and the Formation of Attachment: Most developmental psychologists argue that a child becomes securely attached when there is consistent contact from one or more caregivers who meet the physical and emotional needs of the child in a responsive and appropriate manner. However, even in cultures where mothers do not talk, cuddle, and play with their infants, secure attachments can develop (LeVine et. al., 1994).
The insecure ambivalent style occurs when the parent is insensitive and responds inconsistently to the child’s needs. Consequently, the infant is never sure that the world is a trustworthy place or that he or she can rely on others without some anxiety. A caregiver who is unavailable, perhaps because of marital tension, substance abuse, or preoccupation with work, may send a message to the infant he or she cannot rely on having needs met. An infant who receives only sporadic attention when experiencing discomfort may not learn how to calm down. The child may cry if separated from the caregiver and also cry upon their return. They seek constant reassurance that never seems to satisfy their doubt. Keep in mind that clingy behavior can also just be part of a child’s natural disposition or temperament and does not necessarily reflect some kind of parental neglect. Additionally, a caregiver that attends to a child’s frustration can help teach them to be calm and to relax.
The insecure-avoidant style is marked by insecurity, but this style is also characterized by a tendency to avoid contact with the caregiver and with others. This child may have learned that needs typically go unmet and learns that the caregiver does not provide care and cannot be relied upon for comfort, even sporadically. An insecure-avoidant child learns to be more independent and disengaged.
The insecure disorganized/disoriented style represents the most insecure style of attachment and occurs when the child is given mixed, confused, and inappropriate responses from the caregiver. For example, a mother who suffers from schizophrenia may laugh when a child is hurting or cry when a child exhibits joy. The child does not learn how to interpret emotions or to connect with the unpredictable caregiver. This type of attachment is also often seen in children who have been abused. Research has shown that abuse disrupts a child’s ability to regulate their emotions (Main & Solomon, 1990).
Caregiver Consistency: Having a consistent caregiver may be jeopardized if the infant is cared for in a day care setting with a high turn-over of staff or if institutionalized and given little more than basic physical care. Infants who, perhaps because of being in orphanages with inadequate care, have not had the opportunity to attach in infancy may still form initial secure attachments several years later. However, they may have more emotional problems of depression, anger, or be overly friendly as they interact with others (O’Connor et. al., 2003).

Social Deprivation: Severe deprivation of parental attachment can lead to serious problems. According to studies of children who have not been given warm, nurturing care, they may show developmental delays, failure to thrive, and attachment disorders (Bowlby, 1982). Non-organic failure to thrive is the diagnosis for an infant who does not grow, develop, or gain weight on schedule and there is no known medical explanation for this failure. Poverty, neglect, inconsistent parenting, and severe family dysfunction are correlated with non-organic failure to thrive. In addition, postpartum depression can cause even a well-intentioned mother to neglect her infant.
Reactive Attachment Disorder: Children who experience social neglect or deprivation, repeatedly change primary caregivers that limit opportunities to form stable attachments or are reared in unusual settings (such as institutions) that limit opportunities to form stable attachments can certainly have difficulty forming attachments. According to the Diagnostic and Statistical Manual of Mental Disorders, 5th edition (American Psychiatric Association, 2013), those children experiencing neglectful situations and also displaying markedly disturbed and developmentally inappropriate attachment behavior, such as being inhibited and withdrawn, minimal social and emotional responsiveness to others, and limited positive affect, may be diagnosed with reactive attachment disorder. This disorder often occurs with developmental delays, especially in cognitive and language areas. Fortunately, the majority of severely neglected children do not develop reactive attachment disorder, which occurs in less than 10% of such children. The quality of the caregiving environment after serious neglect affects the development of this disorder.
Resiliency: Being able to overcome challenges and successfully adapt is resiliency. Even young children can exhibit strong resiliency to harsh circumstances. Resiliency can be attributed to certain personality factors, such as an easy-going temperament. Some children are warm, friendly, and responsive, whereas others tend to be more irritable, less manageable, and difficult to console, and these differences play a role in attachment (Gillath, Shaver, Baek, & Chun, 2008; Seifer, Schiller, Sameroff, Resnick, & Riordan, 1996). It seems safe to say that attachment, like most other developmental processes, is affected by an interplay of genetic and socialization influences.
Receiving support from others also leads to resiliency. A positive and strong support group can help a parent and child build a strong foundation by offering assistance and positive attitudes toward the newborn and parent. In a direct test of this idea, Dutch researcher van den Boom (1994) randomly assigned some babies’ mothers to a training session in which they learned to better respond to their children’s needs. The research found that these mothers’ babies were more likely to show a secure attachment style in comparison to the mothers in a control group that did not receive training.
Erikson: Autonomy vs. Shame and Doubt
As the child begins to walk and talk, an interest in independence or autonomy replaces a concern for trust. The toddler tests the limits of what can be touched, said, and explored. Erikson (1982) believed that toddlers should be allowed to explore their environment as freely as safety allows and in so doing will develop a sense of independence that will later grow to self-esteem, initiative, and overall confidence. If a caregiver is overly anxious about the toddler’s actions for fear that the child will get hurt or violate other’s expectations, the caregiver can give the child the message that he or she should be ashamed of their behavior and instill a sense of doubt in their own abilities. Parenting advice based on these ideas would be to keep toddlers safe but let them learn by doing.
Measuring Infant Development
The Bayley Scales of Infant and Toddler Development, Third Edition (Bayley-III) comprehensively assess children within the age range of 1 to 42 months (Pearson Education, 2016). Children are evaluated in five key developmental domains, including cognition, language, social-emotional, motor, and adaptive behavior. By identifying developmental delays in the very young, the Bayley Scales can highlight which early intervention techniques might be most beneficial. Detailed information is even able to be obtained from non-verbal children.
References
Ainsworth, M. (1979). Infant-mother attachment. American Psychologist, 34(10), 932-937.
Ainsworth, M., Blehar, M., Waters, E., & Wall, S. (1978). Patterns of attachment. Hillsdale, NJ: Erlbaum.
Akimoto, S. A., & Sanbinmatsu, D. M. (1999). Differences in self-effacing behavior between European and Japanese Americans: Effect on competence evaluations. Journal of Cross-Cultural Psychology, 30, 159-177.
American Optometric Association. (2019). Infant vision: Birth to 24 months of age. Retrieved from https://www.aoa.org/patients-and-public/good-vision-throughout-life/childrens-vision/infant-vision-birth-to-24- months-of-age
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders, 5th edition (DSM-5).
Washington, DC: Author.
Anglin, J. M. (1993). Vocabulary development: A morphological analysis. Monographs of the Society for Research in Child Development, 58 10), v–165.
Aslin, R. N. (1981). Development of smooth pursuit in human infants. In D. F. Fisher, R. A. Monty, & J. W. Senders (Eds.), Eye movements: Cognition and visual perception (pp. 31– 51). Hillsdale, NJ: Erlbaum.
Atkinson, J., & Braddick, O. (2003). Neurobiological models of normal and abnormal visual development. In M. de Haan & M. H. Johnson (Eds.), The cognitive neuroscience of development (pp. 43– 71). Hove: Psychology Press.
Baillargeon, R. (1987. Object permanence in 3 ½ and 4 ½ year-old infants. Developmental Psychology, 22, 655-664. Baillargeon, R., Li, J., Gertner, Y, & Wu, D. (2011). How do infants reason about physical events? In U. Goswami (Ed.), The Wiley-Blackwell handbook of childhood cognitive development. MA: John Wiley.
Balaban, M. T. & Reisenauer, C. D. (2013). Sensory development. In N. J. Salkind (Ed.), Encyclopedia of human development (pp. 1144-1147). New, York: Sage Publications.
Baldwin, D. A. (1993). Early referential understanding: Infants’ ability to recognize referential acts for what they are. Developmental Psychology, 29(5), 832–843.
Bandura, A. (1977). Social learning theory. Englewood Cliffs, NJ: Prentice Hall.
Bartrip J, Morton J, & De Schonen S. (2001). Responses to mother’s face in 3-week to 5-month-old infants. British Journal of Developmental Psychology, 19, 219–232
Berk, L. E. (2007). Development through the life span (4th ed.). Boston: Allyn and Bacon.
Berne, S. A. (2006). The primitive reflexes: Considerations in the infant. Optometry & Vision Development, 37(3), 139-145. Bloem, M. (2007). The 2006 WHO child growth standards. BMJ : British Medical Journal, 334(7596), 705–706. http://doi.org/10.1136/bmj.39155.658843.BE
Blossom, M., & Morgan, J. L. (2006). Does the face say what the mouth says? A study of infants’ sensitivity to visual prosody. In the 30th annual Boston University conference on language development, Somerville, MA.
Bogartz, R. S., Shinskey, J. L., & Schilling, T. (2000). Object permanence in five-and-a-half month old infants. Infancy, 1(4), 403-428.
Bowlby, J. (1969). Attachment and loss. London: Hogarth Press. Bowlby, J. (1982). Attachment (2nd ed.). New York: Basic Books.
Bradshaw, D. (1986). Immediate and prolonged effectiveness of negative emotion expressions in inhibiting infants’ actions (Unpublished doctoral dissertation). Berkeley, CA: University of California, Berkeley.
Braungart-Rieker, J. M., Hill-Soderlund, A. L., &Karrass, J. (2010). Fear, anger reactivity trajectories from 4 to 16 months: The roles of temperament, regulation, and maternal sensitivity. Developmental Psychology, 46, 791-804.
Bushnell, I. W. R. (2001) Mother’s face recognition in newborn infants: Learning and memory. Infant Child Development, 10, 67-94.
Bushnell, I. W. R., Sai, F., Mullin, J. T. (1989). Neonatal recognition of mother’s face. British Journal of Developmental Psychology, 7, 3-15.
Bruer, J. T. (1999). The myth of the first three years: A new understanding of early brain development and lifelong learning. New York: Simon and Schuster.
Campanella, J., & Rovee-Collier, C. (2005). Latent learning and deferred imitation at 3 months. Infancy, 7(3), 243-262. Carlson, N. (2014). Foundations of behavioral neuroscience (9th ed.). Boston, MA: Pearson.
Carpenter, R., McGarvey, C., Mitchell, E. A., Tappin, D. M., Vennemann, M. M., Smuk, M., & Carpenter, J. R. (2013). Bed sharing when parents do not smoke: Is there a risk of SIDS? An individual level analysis of five major case–control studies. BMJ Open, 3:e002299. doi:10.1136/bmjopen-2012-002299
Centers for Disease Control and Prevention. (2018). Breastfeeding facts. Retrieved from https://www.cdc.gov/breastfeeding/data/facts.html
Centers for Disease Control and Prevention. (2019). Sudden unexpected infant death and sudden infant death syndrome. Retrieved from http://www.cdc.gov/sids/data.htm
Cheour-Luhtanen, M., Alho. K., Kujala, T., Reinikainen, K., Renlund, M., Aaltonen, O., … & Näätänen R. (1995). Mismatch negativity indicates vowel discrimination in newborns. Hearing Research, 82, 53–58.
Chess, S., & Thomas, A. (1996). Temperament: Theory and practice. New York: Brunner/Mazel.
Chi, J. G., Dooling, E. C., & Gilles, F. H. (1977). Left-right asymmetries of the temporal speech areas of the human fetus. Archives of Neurology, 34, 346–8.
Chien S. (2011). No more top-heavy bias: Infants and adults prefer upright faces but not top-heavy geometric or face-like patterns. Journal of Vision, 11(6):1–14.
Chomsky, N. (1965). Aspects of the theory of syntax. Cambridge, MA: MIT Press. Chomsky, N. (1972). Language and mind. NY: Harcourt Brace.
Clark, E. V. (2009). What shapes children’s language? Child-directed speech and the process of acquisition. In V. C. M. Gathercole (Ed.), Routes to language: Essays in honor of Melissa Bowerman. NY: Psychology Press.
Clark, L. A., Kochanska, G., & Ready, R. (2000). Mothers’ personality and its interaction with child temperament as predictors of parenting behavior. Journal of Personality and Social Psychology, 79, 274–285.
Clemson University Cooperative Extension. (2014). Introducing solid foods to infants. Retrieved from http://www.clemson.edu/extension/hgic/food/nutrition/nutrition/life_stages/hgic4102.html
Cole, P. M., Armstrong, L. M., & Pemberton, C. K. (2010). The role of language in the development of emotional regulation. In S. D. Calkins & M. A. Bell (Eds.). Child development at intersection of emotion and cognition (pp. 59-77). Washington D.C.: American Psychological Association.
Colvin, J.D., Collie-Akers, V., Schunn, C., & Moon, R.Y. (2014). Sleep environment risks for younger and older infants. Pediatrics Online. Retrieved from http://pediatrics.aappublications.org/content/pediatrics/early/2014/07/09/peds. 2014-0401.full.pdf
Crain, W. (2005). Theories of development concepts and applications (5th ed.). NJ: Pearson.
de Boysson-Bardies, B., Sagart, L., & Durand, C. (1984). Discernible differences in the babbling of infants according to target language. Journal of Child Language, 11(1), 1–15.
DeCasper, A. J., & Fifer, W. P. (1980). Of human bonding: Newborns prefer their mother’s voices. Science, 208, 1174-1176. DeCasper, A. J., & Spence, M. J. (1986). Prenatal maternal speech influences newborns’ perception of speech sounds. Infant Behavior and Development, 9, 133-150.
Diamond, A. (1985). Development of the ability to use recall to guide actions, as indicated by infants’ performance on AB. Child Development, 56, 868-883.
Dobrich, W., & Scarborough, H. S. (1992). Phonological characteristics of words young children try to say. Journal of Child Language, 19(3), 597–616.
Dubois, J., Hertz-Pannier, L., Cachia, A., Mangin, J. F., Le Bihan, D., & Dehaene-Lambertz, G. (2009). Structural asymmetries in the infant language and sensori-motor networks. Cerebral Cortex, 19, 414–423.
Eisenberg, A., Murkoff, H. E., & Hathaway, S. E. (1989). What to expect the first year. New York: Workman Publishing.
Eisenberg, N., Fabes, R. A., Shepard, S. A., Guthrie, I.K., Murphy, B.C., & Reiser, M. (1999). Parental reactions to children’s negative emotions: Longitudinal relations to quality of children’s social functioning. Child Development, 70, 513-534.
Eisenberg, N., Hofer, C., Spinrad, T., Gershoff, E., Valiente, C., Losoya, S. L., Zhou, Q., Cumberland, A., Liew, J., Reiser, M., & Maxon, E. (2008). Understanding parent-adolescent conflict discussions: Concurrent and across-time prediction from youths’ dispositions and parenting. Monographs of the Society for Research in Child Development, 73, (Serial No. 290, No. 2), 1-160.
El-Dib, M., Massaro, A. N., Glass, P., & Aly, H. (2012). Neurobehavioral assessment as a predictor of neurodevelopmental outcome in preterm infants. Journal of Perinatology, 32, 299-303.
Eliot, L. (1999). What’s going on in there? New York: Bantam. Erikson, E. (1982). The life cycle completed. NY: Norton & Company.
Evans, N., & Levinson, S. C. (2009). The myth of language universals: Language diversity and its importance for cognitive science. Behavioral and Brain Sciences, 32(5), 429–448.
Farroni, T., Johnson, M.H. Menon, E., Zulian, L. Faraguna, D., Csibra, G. (2005). Newborns’ preference for face-relevant stimuli: Effects of contrast polarity. Proceedings of the National Academy of Sciences of the United States of America, 102(47), 17245-17250.
Fergusson, D. M., & Woodward, L. J. (1999). Breastfeeding and later psychosocial adjustment. Paediatric and Perinatal Epidemiology, 13, 144-157.
Fitzpatrick, E.M., Crawford, L., Ni, A., & Durieux-Smith, A. (2011). A descriptive analysis of language and speech skills in 4-to- 5-yr-old children with hearing loss. Ear and Hearing, 32(2), 605-616.
Freud, S. (1938). An outline of psychoanalysis. London: Hogarth.
Galler J. R., & Ramsey F. (1989). A follow-up study of the influence of early malnutrition on development: Behavior at home and at school. American Academy of Child and Adolescence Psychiatry, 28 (2), 254-61.
Galler, J. R., Ramsey, F. C., Morely, D. S., Archer, E., & Salt, P. (1990). The long-term effects of early kwashiorkor compared with marasmus. IV. Performance on the national high school entrance examination. Pediatric Research, 28(3), 235- 239.
Galler, J. R., Ramsey, F. C., Salt, P. & Archer, E. (1987). The long-term effect of early kwashiorkor compared with marasmus. III. Fine motor skills. Journal of Pediatric Gastroenterology Nutrition, 6, 855-859.
Giedd, J. N. (2015). The amazing teen brain. Scientific American, 312(6), 32-37.
Giles, A., & Rovee-Collier, C. (2011). Infant long-term memory for associations formed during mere exposure. Infant Behavior and Development, 34 (2), 327-338.
Gillath, O., Shaver, P. R., Baek, J. M., & Chun, D. S. (2008). Genetic correlates of adult attachment style. Personality & Social Psychology Bulletin, 34, 1396–1405.
Gleitman, L. R., & Newport, E. L. (1995). The invention of language by children: Environmental and biological influences on the acquisition of language. An Invitation to Cognitive Science, 1, 1-24.
Goldin-Meadow, S., & Mylander, C. (1998). Spontaneous sign systems created by deaf children in two cultures. Nature, 391(6664), 279–281.
Grosse, G., Behne, T., Carpenter, M., & Tomasello, M. (2010). Infants communicate in order to be understood. Developmental Psychology, 46(6), 1710-1722.
Gunderson, E. P., Hurston, S. R., Ning, X., Lo, J. C., Crites, Y., Walton, D…. & Quesenberry, C. P. Jr. (2015). Lactation and progression to type 2 diabetes mellitus after gestational diabetes mellitus: A prospective cohort study. American Journal of Medicine, 163, 889-898. Doi: 10.7326/m 15-0807.
Hainline L. (1978). Developmental changes in visual scanning of face and nonface patterns by infants. Journal of Experimental Child Psychology, 25, 90–115.
Hamer, R. (2016). The visual world of infants. Scientific American, 104, 98-101. Harlow, H. F. (1958). The nature of love. American Psychologist, 13, 673-685.
Harris, Y. R. (2005). Cognitive development. In N. J. Salkind (Ed.), Encyclopedia of human development (pp. 276-281). New, York: Sage Publications.
Hart, S., & Carrington, H. (2002). Jealousy in 6-month-old infants. Infancy, 3(3), 395-402.
Hatch, E. M. (1983). Psycholinguistics: A second language perspective. Rowley, MA: Newbury House Publishers. Hertenstein, M. J., & Campos, J. J. (2004). The retention effects of an adult’s emotional displays on infant behavior. Child Development, 75(2), 595–613.
Holland, D., Chang, L., Ernst, T., Curan, M Dale, A. (2014). Structural growth trajectories and rates of change in the first 3 months of infant brain development. JAMA Neurology, 71(10), 1266-1274.
Huttenlocher, P. R., & Dabholkar, A. S. (1997). Regional differences in synaptogenesis in human cerebral cortex. The Journal of Comparative Neurology, 387(2), 167-178.
Hyde, J. S., Else-Quest, N. M., & Goldsmith, H. H. (2004). Children’s temperament and behavior problems predict their employed mothers’ work functioning. Child Development, 75, 580–594.
Hyvärinen, L., Walthes, R., Jacob, N., Nottingham Chaplin, K., & Leonhardt, M. (2014). Current understanding of what infants see. Current Opthalmological Report, 2, 142-149. doi:10.1007/s40135-014-0056-2
Imai, M., Li, L., Haryu, E., Hirsh-Pasek, K., Golinkoff, R. M., & Shigematsu, J. (2008). Novel noun and verb learning in Chinese, English, and Japanese children: Universality and language-specificity in novel noun and verb learning. Child Development, 79, 979-1000.
Islami, F., Liu, Y., Jemal, A., Zhou, J., Weiderpass, E., Colditz, G…Weiss, M. (2015). Breastfeeding and breast cancer risk by receptor status – a systematic review and meta-analysis. Annals of Oncology, 26, 2398-2407.
Iverson, J. M., & Goldin-Meadow, S. (2005). Gesture paves the way for language development. Psychological science, 16(5), 367-371.
Jarrett, C. (2015). Great myths of the brain. West Sussex, UK: Wiley.
Johnson, M. H., & deHaan, M. (2015). Developmental cognitive neuroscience: An introduction. Chichester, West Sussex: UK, Wiley & Sons
Jusczyk, P.W., Cutler, A., & Redanz, N.J. (1993). Infants’ preference for the predominant stress patterns of English words. Child Development, 64, 675–687.
Karlson, E.W., Mandl, L.A., Hankison, S. E., & Grodstein, F. (2004). Do breast-feeding and other reproductive factors influence future risk of rheumatoid arthritis? Arthritis & Rheumatism, 50 (11), 3458-3467.
Kasprian, G., Langs, G., Brugger, P. C., Bittner, M., Weber, M., Arantes, M., & Prayer, D. (2011). The prenatal origin of hemispheric asymmetry: an in utero neuroimaging study. Cerebral Cortex, 21, 1076–1083.
Kiff, C. J., Lengua, L. J., & Zalewski, M. (2011). Nature and nurturing: Parenting in the context of child temperament. Clinical Child and Family Psychology Review, 14, 251–301. doi: 10.1007/s10567-011-0093-4
Klein, P. J., & Meltzoff, A. N. (1999). Long-term memory, forgetting, and deferred imitation in 12-month-old infants. Developmental Science, 2(1), 102-113.
Klinnert, M. D., Campos, J. J., & Sorce, J. F. (1983). Emotions as behavior regulators: Social referencing in infancy. In R. Plutchik & H. Kellerman (Eds.), Emotion: Theory, research, and experience (pp. 57–86). New York, NY: Academic Press.
Kolb, B., & Fantie, B. (1989). Development of the child’s brain and behavior. In C. R. Reynolds & E. Fletcher-Janzen (Eds.),
Handbook of clinical child neuropsychology (pp. 17–39). New York, NY: Plenum Press.
Kolb, B. & Whishaw, I. Q. (2011). An introduction to brain and behavior (3rd ed.). New York: Worth Publishers.
Kopp, C. B. (2011). Development in the early years: Socialization, motor development, and consciousness. Annual Review of Psychology, 62, 165-187.
Latham, M. C. (1997). Human nutrition in the developing world. Rome, IT: Food and Agriculture Organization of the United Nations.
Lavelli, M., & Fogel, A. (2005). Developmental changes in the relationships between infant attention and emotion during early face-to-face communications: The 2 month transition. Developmental Psychology, 41, 265-280.
Lenneberg, E. (1967). Biological foundations of language. New York, NY: John Wiley & Sons.
LeVine, R. A., Dixon, S., LeVine, S., Richman, A., Leiderman, P. H., Keefer, C. H., & Brazelton, T. B. (1994). Child care and culture: Lessons from Africa. New York: Cambridge University Press.
Lewis, M., & Brooks, J. (1978). Self-knowledge and emotional development. In M. Lewis & L. A. Rosenblum (Eds.), Genesis of behavior (Vol. 1, pp. 205-226). New York: Plenum Press.
Lewis, T. L., Maurer, D., & Milewski, A. (1979). The development of nasal detection in young infants. Investigative Ophthalmology and Visual Science Supplement, 19, 271.
Li, Y., & Ding, Y. (2017). Human visual development. In Y. Liu., & W. Chen (Eds.), Pediatric lens diseases (pp. 11-20). Singapore: Springer.
Los Angles County Department of Public Health. (2019). Breastfeeding vs. formula feeding. Retrieved from http://publichealth.lacounty.gov/LAmoms/lessons/Breastfeeding/6_BreastfeedingvsFormulaFeeding.pdf
Main, M., & Solomon, J. (1990). Procedures for identifying infants as disorganized/disoriented during the Ainsworth Strange Situation. In M. T. Greenberg, D. Cicchetti, & E. M. Cummings (Eds.), Attachment inthe Preschool Years (pp.121– 160).Chicago,IL: UniversityofChicagoPress.
Mandel, D. R., Jusczyk, P. W., & Pisoni, D. B. (1995). Infants’ recognition of the sound patterns of their own names. Psychological Science, 6(5), 314–317.
Mayberry, R. I., Lock, E., & Kazmi, H. (2002). Development: Linguistic ability and early language exposure. Nature, 417(6884), 38.
Moeller, M.P., & Tomblin, J.B. (2015). An introduction to the outcomes of children with hearing loss study. Ear and Hearing, 36 Suppl (0-1), 4S-13S
Morelli, G., Rogoff, B., Oppenheim, D., & Goldsmith, D. (1992). Cultural variations in infants’ sleeping arrangements: Questions of independence. Developmental Psychology, 28, 604-613.
Nelson, E. A., Schiefenhoevel, W., & Haimerl, F. (2000). Child care practices in nonindustrialized societies. Pediatrics, 105, e75.
O’Connor, T. G., Marvin, R. S., Rotter, M., Olrich, J. T., Britner, P. A., & The English and Romanian Adoptees Study Team. (2003). Child-parent attachment following early institutional deprivation. Development and Psychopathology, 15, 19- 38.
Papousek, M. (2007). Communication in early infancy: An arena of intersubjective learning. Infant Behavior and Development, 30, 258-266.
Pearson Education. (2016). Bayley Scales of Infant Development, Third Edition. New York: Pearson. Retrieved from http://www.pearsonclinical.com/childhood/products/100000123/bayley-scales-of-infant-and-toddler-development- third-edition-bayley-iii.html#tab-details
Penfield, W., & Roberts, L. (1959). Speech and brain mechanisms. Princeton, NJ: Princeton University Press.
Petitto, L. A., & Marentette, P. F. (1991). Babbling in the manual mode: Evidence for the ontogeny of language. Science, 251(5000), 1493–1496.
Phelps, B. J. (2005). Habituation. In N. J. Salkind (Ed.), Encyclopedia of human development (pp. 597-600). New York: Sage Publications.
Piaget, J. (1954). The construction of reality in the child. New York: Basic Books.
Pickens, J., Field, T., Nawrocki, T., Martinez, A., Soutullo, D., & Gonzalez, J. (1994). Full-term and preterm infants’ perception of face-voice synchrony. Infant Behavior and Development, 17(4), 447-455.
Porter, R. H., Makin, J. W., Davis, L. M., Christensen, K. (1992). Responsiveness of infants to olfactory cues from lactating females. Infant Behavior and Development, 15, 85-93.
Redondo, C. M., Gago-Dominguez, M., Ponte, S. M., Castelo, M. E., Jiang, X., Garcia, A.A… Castelao, J. E. (2012). Breast feeding, parity and breast cancer subtypes in a Spanish cohort. PLoS One, 7(7): e40543 doi: 10.1371/journal.pone.00040543
Richardson, B. D. (1980). Malnutrition and nutritional anthropometry. Journal of Tropical Pediatrics, 26(3), 80-84. Rothbart, M. K., & Bates, J. E. (2006). Temperament. In N. Eisenberg (Ed.). Handbook of child psychology: Vol. 3: Social, emotional, and personality development (6th ed., pp. 99-116). Hoboken, NJ: Wiley.
Rothbart, M. K., Posner, M. I. & Kieras, J. (2006). Temperament, attention, and the development of self-regulation. In M. McCartney & D. Phillips (Eds.) Blackwell handbook of early childhood development (pp. 3338-357). Malden, MA: Blackwell.
Rothbaum, F., Weisz, J., Pott, M., Miyake, K., & Morelli, G. (2010). Attachment and culture: Security in the United States and Japan. American Psychologist, 55, 1093-1104.
Rovee-Collier, C. (1987). Learning and memory in infancy. In J. D. Osofsky (Ed.), Handbook of infant development, (2nd, ed., pp. 98-148). New York: Wiley.
Rovee-Collier, C. (1990). The “memory system” of prelinguistic infants. Annuals of the New York Academy of Sciences, 608, 517-542. doi: 10.1111/j.1749-66231990.tb48908.
Rovee-Collier, C., & Hayne, H. (1987). Reactivation of infant memory: Implications for cognitive development. In H. W. Reese (Ed.), Advances in child development and behavior. (Vol. 20, pp. 185-238). London, UK: Academic Press.
Rymer, R. (1993). Genie: A scientific tragedy. Harmondsworth: Penguin.
Salkind, N. J. (2005). Encyclopedia of human development. New York: Sage Publications.
Schwarz, E. B., Brown, J. S., Creasman, J. M. Stuebe, A., McClure, C. K., Van Den Eeden, S. K., & Thom, D. (2010). Lactation and maternal risk of type-2 diabetes: A population-based study. American Journal of Medicine, 123, 863.e1-863.e6. doi: 10.1016/j.amjmed.2010.03.016.
Seifer, R., Schiller, M., Sameroff, A., Resnick, S., & Riordan, K. (1996). Attachment, maternal sensitivity, and infant temperament during the first year of life. Developmental Psychology, 32, 12-25.
Sen, M. G., Yonas, A., & Knill, D. C. (2001). Development of infants’ sensitivity to surface contour information for spatial layout. Perception, 30, 167-176.
Senghas, R. J., Senghas, A., & Pyers, J. E. (2005). The emergence of Nicaraguan Sign Language: Questions of development, acquisition, and evolution. In S. T. Parker, J. Langer, & C. Milbrath (Eds.), Biology and knowledge revisited: From neurogenesis to psychogenesis (pp. 287–306). Mahwah, NJ: Lawrence Erlbaum Associates.
Shaffer, D. R. (1985). Developmental psychology: Theory, research, and applications. Belmont, CA: Wadsworth, Inc. Skinner, B. F. (1953). Science and human behavior. NY: Free Press.
Sorce, J. F., Emde, J. J., Campos, J. J., & Klinnert, M. D. (1985). Maternal emotional signaling: Its effect on the visual cliff behavior of 1-year-olds. Developmental Psychology, 21, 195–200.
Spelke, E. S., & Cortelyou, A. (1981). Perceptual aspects of social knowing: Looking and listening in infancy. Infant social cognition, 61-84.
Springer, S. P. & Deutsch, G. (1993). Left brain, right brain (4th ed.). New York: W. H. Freeman.
Stika, C.J., Eisenberg, L.S., Johnson, K.C. Henning, S.C., Colson, B.G., Ganguly, D.H., & DesJardin, J.L. (2015). Developmental outcomes of early-identified children who are hard of hearing at 12 to 18 months of age. Early Human Development, 9(1), 47-55.
Stork, F. & Widdowson, J. (1974). Learning about Linguistics. London: Hutchinson.
Thomas, R. M. (1979). Comparing theories of child development. Santa Barbara, CA: Wadsworth.
Thompson, R. A. (2006). The development of the person. In W. Damon & R. Lerner (Eds.), Handbook of child psychology (6th Ed.). New York: Wiley.
Thompson, R. A., & Goodvin, R. (2007). Taming the tempest in the teapot. In C. A. Brownell & C. B. Kopp (Eds.). Socioemotional development in the toddler years: Transitions and transformations (pp. 320-342). New York: Guilford.
Thompson, R. A., Winer, A. C., & Goodvin, R. (2010). The individual child: Temperament, emotion, self, and personality. In M. Bornstein & M. E. Lamb (Eds.), Developmental science: An advanced textbook (6th ed., pp. 423–464). New York, NY: Psychology Press/Taylor & Francis.
Titus-Ernstoff, L., Rees, J. R., Terry, K. L., & Cramer, D. W. (2010). Breast-feeding the last-born child and risk of ovarian cancer. Cancer Causes Control, 21(2), 201-207. doi: 10.1007/s10552-009-9450-8
Tomblin, J. B., Harrison, M., Ambrose, S. E., Walker, E. A., Oleson, J. J., & Moeller, M. P. (2015). Language outcomes in young children with mild to severe hearing loss. Ear and hearing, 36 Suppl 1(0 1), 76S–91S.
United Nations Children’s Fund. (2015). Levels and trends in child mortality: Report 2015. United Nations Children’s Fund. New York: NY.
United States Department of Health and Human Services, Office of Women’s Health. (2011). Your guide to breast feeding. Washington D.C.
United States National Library of Medicine. (2016). Circumcision. Retrieved from https://medlineplus.gov/circumcision.html
Van den Boom, D. C. (1994). The influence of temperament and mothering on attachment and exploration: An experimental manipulation of sensitive responsiveness among lower-class mothers with irritable infants. Child Development, 65, 1457–1477.
Van Ijzendoorn, M. H., & Sagi, A. (1999). Cross-cultural patterns of attachment. In J. Cassidy & P. R. Shaver (Eds.), Handbook of attachment: Theory, research, and clinical applications (pp. 713-734). New York: Guilford.
Webb, S. J., Monk, C. S., & Nelson, C. A. (2001). Mechanisms of postnatal neurobiological development: Implications for human development. Developmental Neuropsychology, 19, 147-171.
Weekes-Shackelford, V. A. & Shackelford, T. K. (2005). Sudden Infant Death Syndrome (SIDS). In N. J. Salkind (Ed.), Encyclopedia of human development (pp. 1238-1239). New York: Sage Publications.
Werker, J. F., Pegg, J. E., & McLeod, P. J. (1994). A cross-language investigation of infant preference for infant-directed communication. Infant Behavior and Development, 17, 323-333.
Werker, J. F., & Tees, R. C. (2002). Cross-language speech perception: Evidence for perceptual reorganization during the first year of life. Infant Behavior and Development, 25, 121-133.
Attribution
Adapted from Chapter 3 from Lifespan Development: A Psychological Perspective Second Edition by Martha Lally and Suzanne Valentine-French under the Creative Commons Attribution-Noncommercial-Share Alike 3.0 unported license.
