Chapter 31: Substance Abuse
Learning Objectives
- Learn from the national and global perspectives of substance abuse among immigrants and refugees.
- Recognizing that the world is constantly and rapidly changing.
- Recognizing that Global/national/international events can have an impact on individuals, families, groups, organizations, and communities.
- Global implications dictate that we foster international relationships and opportunities to address international concerns, needs, problems, and actions to improve the well-being of not only U.S. citizens, but global citizens.
33.1 Introduction
“The area we are living [in] is very, very bad. . . . So the kids you cannot discipline them . . . they’re going to school, the kids are smoking weed, there are drug-addicted kids . . . But I don’t have a choice because that’s where I live and that’s where they go to school.”
– Somali Refugee mother (Betancourt et al., 2015, p. 117)
Substance abuse occurs among every community, regardless of race, ethnicity, culture, country of origin, and socioeconomic status. Immigrants and refugees living in the in the United States are no different. However, the resettlement process adds additional complexities to understanding how immigrant and refugee communities are impacted by substance abuse. Immigrants have acquired habits and customs of substance use from their home country, and they must navigate these customs and any clashes with local United States customs. Additionally, immigrants often face limited employment and housing options, which means they may be unable to leave neighborhoods with prevalent substance use (as in the example above). Immigrants frequently have stressors associated with scarce employment, the need to send money to family, past traumatic exposure, and separation from family. Some immigrant and refugee groups may be at greater risk for abusing substances as a means of coping with these stressors. However, immigrants also have significant protective factors, such as specific cultural norms and family support.
Upon entering the United States, immigrants are at lower risk of alcohol abuse than United States-born citizens, even in comparison to those with the same ethnic identity (Breslau & Chang, 2006; Escobar, Nervi, & Gara, 2000). Research has also found that for immigrants, there is a positive correlation between the length of stay in the United States and the increased risk of alcohol abuse (Szaflarski, Cubbins, & Ying, 2011). This may be due to protective factors shared by immigrants or to a lack of culturally validated assessments for substance use in immigrant communities. Understanding the influences of substance abuse within immigrant and refugee populations in the United States is incredibly complex due to two main considerations: (1) the breadth of substances that can be used and abused (e.g., alcohol, tobacco, illicit drugs, and non-prescribed prescription drugs) and (2) the diversity of peoples and cultures that are represented within the United States immigrant and refugee populations.
Definition of substance use disorders:
The American Psychological Association (APA) defines substance abuse disorders as recurrent use of alcohol or drugs that cause significant impairment. Individuals with substance abuse disorders have impaired control, social impairment, risky use, and/or meet pharmacological criteria (2013). There are separate diagnoses by each substance (alcohol, tobacco, cannabis, stimulant, hallucinogen, and opioid). Diagnoses are classified into five categories: use disorder, intoxication, withdrawal, other, substance-induced disorder, and substance-related disorder.
The purpose of this chapter is to more thoroughly explore some of these complexities by utilizing a systemic framework that places problems of substance abuse—within immigrant and refugee communities—within the broader context of families. We begin by reviewing the literature on prevalence and risk factors for substance use among immigrants, followed by an exploration of the specific role of the family. Next, we review the theoretical frameworks on substance abuse, policy, and prevention and intervention models. The scope of this chapter is not to provide a comprehensive review of the substance abuse literature for all immigrant and refugee groups but rather to introduce a general review of the existent research to promote dialogue of current and future research directed at strengthening immigrant and refugee communities within the United States.
Katharine Wickel Didericksen (Medical Family Therapy Program, East Carolina University), Jennifer McCleary (School of Social Work, Tulane University), Nicholas Newstrom (Family Social Science, University of Minnesota), Glenda Mutinda (Medical Family Therapy Program , East Carolina University), & Jaime Ballard (Family Social Science, University of Minnesota).
33.2 Substance Abuse Prevalence
Substance abuse is problematic in every community across the United States, regardless of individual or socioeconomic characteristics. In its far-reaching effects, the estimated costs of substance abuse in the United States is $700 billion annually, with much of the cost related to health care, crime, and loss of work productivity (CDC, 2015; NDIC, 2011; USHHS, 2014). Understanding substance abuse within immigrant populations is becoming increasingly important as the United States increases in cultural diversity (Szaflarski, Cubbins, & Ying, 2011).
In general, immigrants have lower rates of substance use disorders than do United States-born citizens. In a nationally representative sample of adults, prevalence of substance use disorders was substantially lower among first-generation immigrants than among United States-born, and slightly lower among second-generation immigrants than among United States-born (Salas-Wright, Vaughn, Clark, Terzis, & Cordova, 2014). United States-born persons were three to five times more likely to experience lifetime substance abuse or dependence disorders than first-generation immigrants. Specifically, 49% of the United States-born had a lifetime diagnosis of substance abuse or dependence, compared to 18% of first- immigrants.
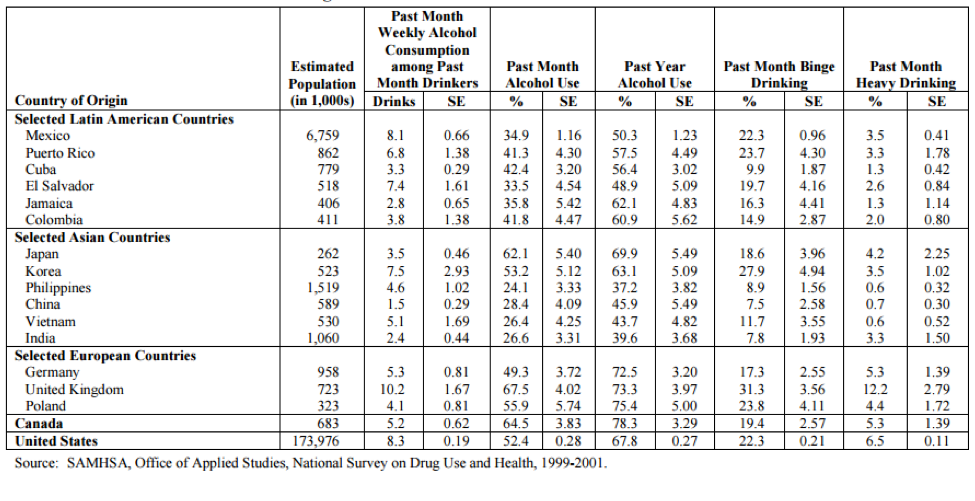
Similarly, a study of immigrant adolescents in Massachusetts found they had a lower risk of alcohol, tobacco, and marijuana use than United States-born adolescents (Almeida, Johnson, Matsumoto, & Godette, 2012). According to the 1999-2001 National Survey on Drug Use and Health, the substance use rates across culture and substance can differ greatly across groups (Brown et al., 2005; see Table 1). These statistics show that understanding substance use and abuse is challenging and complex.
Table 1Estimated numbers and prevalence (with standard errors) of substance consumption in past month and past year among immigrants from selected countries
Prevalence among refugees
Little is known in terms of prevalence statistics of substance abuse in refugee communities in the United States, however in refugee camps, high rates of drug and alcohol use have been reported (Ezard et al., 2011; Luitel, Jordans, Murphy, Roberts, & McCambridge, 2013). In the refugee camps, common substances are alcohol, khat, and cannabis, some made for medicinal purposes and others for recreational use (Streel & Schilperoord, 2010).

Despite these high rates of use in refugee camps, the few studies in the United States have found very low rates of alcohol use and disorders. In a study of substance use among all newly arriving adult refugees in a Texas city, reported rates of current smoking (38.5%) and alcohol use (23%) were very low (Barnes, Harrison, & Heneghan, 2004). The authors note that substance consumption may have been underreported, at least among some ethnicities. The study’s Bosnian interpreter and cultural consultant, for example, believed that the 20% alcohol use rate reported by Bosnians underrepresented use in that community.
Two studies have assessed substance use disorders among refugees. In a national study of refugee children and adolescents receiving treatment through the national child traumatic stress network, less than 4% had a substance use disorder (Betancourt et al., 2012). Similarly, a random sample of Cambodian refugees found that four percent had an alcohol use disorder (Marshall, Schell, Elliott, Berthold, & Chun, 2005).
For refugees, patterns of use differ significantly across the trajectory of displacement. These transitions can be demonstrated in the stories told by Karen refugees (McCleary, 2013; McCleary & Wieling, in press). When the Karen lived in Burma, their country of origin, there were cultural structures that protected most people from harmful alcohol use and consequent problems. However, once people fled to Thailand, alcohol use increased significantly and the problems resulting from harmful use increased. New problems such as violence between unrelated adult men, intimate partner violence, and suicide increased, and were all related to alcohol use. After resettlement, patterns of use changed again. For some people, rates of use increased due to resettlement stress and loss of roles. Alcohol-related problems were worse in the settlement location than in the camps because legal consequences such as DUIs, loss of licenses, fines and jail time were more significant. For other people, alcohol use dropped significantly because harmful alcohol use carried so much more risk (e.g., loss of job, loss of housing, loss of driving privileges). Additionally, in refugee camps, religious and community leaders acted as social supports for many refugees to address alcohol-related problems. However, in the United States, many religious and community leaders feel overwhelmed and unable to support their community members with substance use related concerns.
33.3 Risk Factors
Substances may be used as a means of coping with previous or ongoing trauma, stress, isolation, and uncertainty (Ezard, 2012; United Nations, 2014; Weaver & Roberts, 2010). Each of these phenomena can be a risk factor for substance use and related disorders in immigrant communities. Additionally, particular practices and cultural norms in the country of origin along with acculturation stressors related to local customs in the United States can put immigrants at an increased risk for substance use.
Exposure to traumatic stress and mental health. Many immigrants, particularly refugees, have been exposed to violence and traumatic events in their home countries and during resettlement (Porter & Haslam, 2005; United Nations, 2014). Trauma exposure increases the risk of mental health disorders (Porter & Haslam, 2005; Johnson & Thompson, 2008). Research indicates that some immigrants and refugees are at higher risk for posttraumatic stress disorder (PTSD), anxiety, depression, psychosis, complicated grief and suicide (Akinsulure-Smith & O’Hara, 2012; Birman, & Tran, 2008; Jamil, Hakim-Larson, Farrag, Kafaji, & Jamil, 2002; Jensen, 1996; Kandula Kersey, & Lurie, 2004). These mental health disorders in turn can increase the risk of substance abuse (Ezard, 2012; Weaver & Roberts, 2010). For more information about mental health among immigrants and refugees, see Chapter 5.
However, many immigrants and refugees avoid substance use even after traumatic exposure and distress. In a study of Cambodian refugees 20 years after arrival, alcohol use disorder was positively related to trauma exposure since arriving in the United States, but not to trauma exposure prior to arrival (Marshall, Schell, Elliott, Berthold, & Chun, 2005). A low rate (4%) of alcohol use disorder was found in spite of high rates of PTSD (62%) and major depression disorder (51%) in this community. Similarly, in focus groups conducted with Karen refugees, trauma was described as a much more influential factor in substance use in the refugee camps than in the United States.
Stresses after resettlement. Immigrants face significant stressors as they seek employment and a new life in the United States, particularly when they face discrimination along the way. These stressors are associated with increased substance use. For example, migrant workers report that three of their most common reasons for drinking are isolation from family, boredom, and stress, along with work constraints that lead to lack of dry recreation or opportunities for social connection (Organista, 2007). Furthermore, immigrants’ experiences of unfair treatment and perceived discrimination in finding work are associated with alcohol disorders, prescription drug abuse, and illicit drug use (Gee, Delva, & Takeuchi, 2007).
Immigrants also face stressors linked to the legal consequences of substance use. Within the United States, individuals who abuse alcohol and identify as being from racial minority backgrounds are seen as “doubly vulnerable” (Gwyn & Colin 2010, p. 38). The legal ramifications for racial minority communities are more severe than for majority communities, such as criminal charges (Iguchi, Bell, Ramchand & Fain, 2005) and increased involvement with social service related organizations (i.e., Child Protective Services, Department of Social Services; Roberts & Nuru-Jeter, 2012). Legal proceedings are often expensive and difficult to understand for those without a formal legal education. For people who have language and cultural barriers, this process may become additionally challenging. Immigrants and refugees often experience these additional challenges. Differences in culture, religion, acculturation process, gender roles, hierarchy, collectivism/individualism, and family structures and dynamics often exacerbate the amount of stressors these families face (Rastogi & Wadhwa, 2006). Each of these challenges requires consideration in research, policy, and intervention.
Norms in country of origin and acculturation to local customs. The norms from the country of origin frequently play a role in an immigrant’s substance use and abuse after arrival. For example, in a study of Asian American immigrants, the detrimental drinking pattern (or the “extent to which frequent heavy drinking, drunkenness, festive drinking at community celebrations, drinking with meals, and drinking in public places are common”) in the country of origin was significantly associated with the risk of frequent drunkenness and alcohol-abuse symptoms (Cook, Bond, Karriker-Jaffe, & Zemore, 2013, p. 533). Drinking prevalence (or the “extent to which alcohol consumption is integrated into society as an ordinary occurrence”) in the country of origin was associated with alcohol dependence symptoms (Cook et al., 2013, p. 533). Acculturation to the United States consumption behaviors can also increase the risk of substance abuse (Ezard, 2012; Bacio, Mays, & Lau, 2012; Kam, 2011; Prado et al., 2009). Pumariega, Millsaps, Rodriguez, Moser, & Pumariega (2007), for example, found that adolescents may be at an increased risk of substance abuse due to the challenges of acculturation and adopting ‘Americanized’ activities.

Knowing the various risk factors immigrants face, it is surprising that immigrants report less drug use (i.e., alcohol, cigarette, intravenous drugs, and other illegal drugs) than United States-born individuals (Hussey et al., 2007). This phenomenon of immigrants doing better than United States-born individuals has been termed the immigration paradox (for greater detail, see Chapter 8) because it contradicts assumptions that difficult transitions to a new country increase the likelihood of substance abuse. For example, one study found adolescents in neighborhoods of historical Mexican heritage (e.g., mostly non-immigrants) were at higher risk for alcohol and marijuana use; these neighborhoods tended to have higher rates of crime, poverty, and residential insecurity. However, youth living in neighborhoods that had higher numbers of immigrants reported lower use of alcohol, cigarettes, and marijuana. This suggests that there was something about neighborhoods with more of an immigrant presence that may act as a protective factor in adolescent substance use (Kulis et al., 2007). While this paradox does not hold true for all immigrant groups (Hernandez, Denton, MaCartney, & Blanchard, 2012), many researchers are puzzled at these findings. Recent literature suggests that family support may explain why this is the case.
Video
Sunny Chanthanouvong, Executive Director, Lao Assistance Center of Minnesota, discusses mental health as it relates to migration and resettlement (0:00-2:18).
33.4 Family Influences on Substance Abuse
Family involvement and cohesion are key protective factors for substance abuse among immigrants (Bacio, Mays, & Lau, 2012; Kam, 2011; Prado et al., 2009; Pumariega, Millsaps, Rodriguez, Moser, & Pumariega, 2007). For example, the research team who conducted the neighborhood study addressed above hypothesized that the main protective characteristic against substance use and abuse was family involvement and cohesion. General family and ecological systems theories posit that family members influence each other as they interact on a regular basis. This might be especially true in the case of recently arrived immigrant families who are turn to each other for support.
Parenting style is one strong protective factor. For Latino/a adolescents, parenting style patterns were related to adolescent alcohol use or abstention (Driscoll, Russell, & Crockett, 2008). Driscoll et al. (2008) indicated that there was an increased amount of permissive parenting with successive generations of immigrants, and this parenting style was related to increased alcohol use among adolescents. Those that had authoritative parents did not have an increased risk of alcohol use (Driscoll et al., 2008). This suggests that parenting styles that are high on expectations and support (i.e., authoritative parenting; Baumrind, 1971) may serve as a protective factor against alcohol use for adolescents.
In addition to parenting being important, the general family environment can also influence substance use. For example, Schwartz, Mason, Pantin, & Szapocznik, (2008) indicated that family functioning influenced identity formation, and that adolescents in immigrant families with higher levels of identity confusion were more likely to initiate cigarette and alcohol use, in addition to initiating early sexual experiences. These findings indicate that family functioning can also serve as a protective factor in terms of initiating drug and alcohol behavior. It is important to put this into context as family cohesion pre-immigration has also been negatively correlated with drug use of young adults (Dillon, De La Rosa, Sanchez, & Schwartz, 2012).
The parent-child dyad seems to be of particular importance in the transmission of and uptake of substance abuse (Farrell & White, 1998). Farrel & White (1998) found that when mother-adolescent distress was high, risk of drug use increased among adolescents. In the context of displaced families, while high family cohesion is a protective factor, acculturated adolescents may see this cohesion as a challenge to their independence. If left unresolved, this can become a problem. Conflict between parents and children in immigrant Latinx families predicted lifetime use of alcohol and binge drinking behaviors (Marsiglia, Kulis, Parsai, Villar, & Garcia, 2009). It is important to note that not all families immigrate together and the experience of separation can also impact substance use. For example, when mother-child separates there is an increased risk in terms of drug and alcohol use for adolescents (Mena, Mitrani, Muir, & Santisteban 2008). A second kind of separation can also influence risk factors. Conceptually, this separation relates to ambiguous loss (Boss, 1991), in that they occur when the parent is unable to care for the child due to financial, health (both physical and mental), and substance abuse problems (Mena et al., 2008).
33.5 Theoretical Frameworks
Considering the theoretical background of research about substance abuse among immigrant and refugee populations within the United States is an important part of understanding the current literature; however, there are some difficulties in the conceptualization of theory for these populations within the context of substance abuse. In the existing literature, there are several theories that are used to frame substance abuse within immigrant communities, thus adding to the difficulties as well. It would be unreasonable to expect all authors to subscribe to only one theory, however, the variety of theories found increases the difficulty of a comprehensive discussion. It is beyond the scope of this chapter to mention all of the theories that have been identified to conceptualize this area of literature; instead, a few theoretical frameworks and societal factors that have been used repeatedly in relation to substance abuse and which might be useful in providing additional clarity to these extant complexities will be discussed.
Ecodevelopmental Theory
One approach that has been frequently utilized in the literature is ecodevelopmental theory (Szapocznik & Coatsworth, 1999). This theory takes tenets of ecological systems (Bronfenbrenner, 1977) and developmental theories such as stages highlighted in the expanded family life cycle model (Carter & McGoldrick, 2005) in an attempt to explain the complexities of substance abuse within immigrant and refugee populations. This enables a discussion of surrounding systems that influence the individual, while also taking into account the stages of life many individuals and families experience. For example, Bronfrenbrenner (1977) discussed development as a series of systems that mimicked concentric circles. The circle closest to the individual is the micro-system, which consists of people and environments that influence the individual on a regular basis (i.e., family members, friends, colleagues, work environment, etc.). Each of these micro-systems interacts with each other, and this interaction creates the meso-system. The next two systems are the exo- and macro-systems. The exo-system consists of the larger influences of economics, politics, education, government, and religion, while the macro-system consists of overarching values and beliefs that a person has. This whole system then moves through time and this element of time is termed the chronosystem. Immigrants and refugees may have similar types of micro-systems, however their interaction with their macro-system may be a bit different due to experiences during displacement or migration, language, culture, and law.
The second piece of ecodevelopmental theory is the Family Lifecycle Model. The Family Lifecycle Model describes the normative stages that a family goes through (i.e., initial coupling, marriage/commitment, transitioning to parenthood, etc.). Combining each of these concepts into one theory allows for an understanding of both external and internal influences. Ecological systems theory focuses more on the outside systems with which an individual interacts (i.e., peer and familial influence and work and/or school environment) and the family lifecycle provides an understanding of important internal influences such as stages of life (i.e., childhood, adolescents, coupling, etc.).
Assimilation (or Acculturation) Model
One model that focuses more on the population (i.e., immigrants and refugees) than on the problem (i.e., substance abuse) is the assimilation (or acculturation) model. This model describes newcomers (i.e., immigrants and refugees) as adopting the host country’s customs and patterns of substance use. This means that immigrants and refugees may likely adopt substance use habits that are more reflective of their current surroundings rather than their country of origin. This is not definitive, however, and the literature is mixed. Both D’Avanzo (1997) and Rebhun (1998) reported that people might simply continue the substance abuse patterns that they participated in while living in their country of origin. This may explain the immigrant paradox discussed previously; the longer that immigrants and refugees and their families stay in the United States, the higher their risk for substance abuse. This would make sense as first-generation migrant peoples would have a foreign country of origin, but second-generation would be living in their country of origin and thus only have their current location (with all of its influences, culture, etc.) as a frame of reference.
Biopsychosocial Theory
While the assimilation (or acculturation model) focuses more on the population rather than the problem, the biopsychosocial theory takes another angle. This theory integrates aspects of psychology and sociality to expand the explanation and understanding of biological factors (Engel, 1977), and in utilizing this theory, the problem (substance abuse) is placed as the primary focus. Marlatt (1992) first used this theory to describe substance abuse in an effort to explain the influence of substance abuse on the entirety of a person. According to Marlatt (1992) addictive behaviors are influenced by the combination of biological, psychological, and sociocultural factors. Biological determinants may include genetic predispositions to addiction (Palmer et al., 2015) and the way in which the substance physically affects the body. The biological portion of the experience of substance abuse greatly influences the psychological and social experiences (Marlatt, 1992). Psychological risk may include beliefs or values, mental health, exposure of psychological trauma, and expectations of substance effects. The sociocultural influences include both the influence received from and given to others. Each of these determinants interact with and influence each other, and provide a complex picture of how substance abuse might be experienced.
Health Disparity
Socially disadvantaged populations, such as racial or ethnic minorities, face health disparities. They are more likely to have health problems, less likely to have access to health care, and more likely to receive substandard care (Institute of Medicine, 2002). These disparities result partially from differences in socioeconomic status, education, employment and housing stability. In terms of substance abuse, ethnic minorities are less likely to use or to complete substance abuse treatment (Chartier & Caetano, 2011). This theory suggests that as a disadvantaged population, immigrants and refugees face disparities in access to and use of substance abuse treatment. Consequently, the outcomes of substance use in these populations would be more severe.
Historical Trauma
A historical trauma perspective reminds us that traumatic experiences can lead to wounds that extend across generations (Sotero, 2006). When a community experiences systematic trauma, such as genocide and forced removal from the community, the community as a whole suffers substantial loss and social disadvantages. For example, displacement can lead to reduced socioeconomic status as possessions are left behind and displaced persons must look for employment in a new location. For the individuals in the community, exposure to trauma often leads to psychological symptoms such as PTSD, depression, or anxiety. These trauma-impacted individuals must find a way to cope, and they are likely to turn to substance abuse or other self-destructive behaviors to numb pain. Their parenting and family functioning are likely to be negatively impacted, and their families are likely to be alienated from external supports. These effects will impact their children in turn. Among children of Holocaust survivors, for example, those children who perceived greater parental burden (i.e., the extent to which parents required care from their children due to the parent’s distress from traumatic exposure) had greater symptoms of PTSD (Letzter-Pouw, Shrira, Ben-Ezra, & Palgi, 2014). The children see the ongoing effects of the original trauma.
This framework can be very useful in understanding substance abuse in refugee and other trauma-impacted communities. A refugee community, for example, suffers substantial losses, which impact their ability to function as parents and family members and which increase their chances of turning to substance use to cope with ongoing losses. Children in these families may experience a powerful combination of ineffective parenting, family norms of substance use, socioeconomic disadvantages, and a sense of loss or disconnection related to the original traumatic events and stressors. These children are at risk to turn to substances.
Each of these theories could be helpful in explaining the immigrant or refugee experience of substance abuse. While it is not necessary for a professional to consider using all of these in guiding his/her work, examining each more closely would be beneficial. Each has something to add and to enable consideration of immigrants’ and refugees’ needs regarding substance abuse.
33.6 Policy on Legal Consequences on Substance Abuse
In addition to a host of complexities related to displacement, immigrants to the United States also potentially face additional legal challenges if their behavior is disclosed to the Immigration and Naturalization Service (INS). Substance use can lead to a rejection of an application for admission to the United States, or to deportation. Immigration laws classify three types of substance use: abusers, addicts, and persons convicted of drug-related offenses (Mautino, 2002). While the first two are difficult to determine, for immigrants convictions often result in the individual being deported. Additionally, Mautiono (2002) reports that individuals in any of these three categories may be deemed “inadmissible,” which means that they would not qualify to immigrate to the United States and cannot qualify for a nonimmigrant (temporary) visa (p.1). It is important to note, that if the INS determines an immigrant to be an “abuser” or “addict” the immigrant is deportable without a drug-related conviction (Mautino, 2002). An immigrant is typically labeled as an “abuser” if s/he admits to using at least one illegal substance on one occasion within the past three years (Mautino, 2002). Drug convictions are generally related to possession, transportation, and trafficking illegal substances, and can happen in or outside of the United States; such convictions need not happen within the United States and are cause for deportation or being considered inadmissible (Mautino, 2002).
33.7 Substance Abuse Prevention & Intervention
Substance abuse prevention and intervention programs within the United States are prevalent for both adolescents and adults. However, very few programs have been adapted for specific ethnic groups. There are no programs for refugees that incorporate the additional context of conflict-related displacement. In this section, we address the barriers to substance abuse treatment use among immigrants and refugees, suggestions for professionals providing substance abuse treatment for immigrants and refugees, and programs that have tried to address the barriers to treatment.
Barriers to treatment use and effective treatments. There are many barriers that prevent immigrant and refugee populations from receiving and/or seeking substance abuse treatment. There is common stigmatization of substance abuse, particularly given the potential legal consequences for immigrants determined to be drug abusers. When individuals choose to look into treatment options, they are likely to find a lack of culturally relevant evidence-based treatments and trained providers from various immigrant and refugee backgrounds (e.g., people who identify themselves as members within the community of interest; Amodeo et al., 2004). There may not be limited services available in the immigrant’s language. All of these factors can combine to prevent immigrants and refugees seeking treatment. For example, Arfken, Berry, and Owens (2009) conducted a study to investigate the barriers that prevent Arab Americans from beginning and remaining in substance abuse treatment programs. What they discovered is that the stigma of having a substance abuse problem and seeking treatment as well as language barriers prevented this group from receiving adequate treatment. In poor communities where there’s lack of information, immigrants can also opt not to seek treatment based on inadequate resources for their overall healthcare and their perception of how various laws and policies affect them (Moya & Shedlin, 2008).
In addition to a lack of culturally appropriate treatments and treatment providers, there are few to no culturally appropriate assessments for substance use. Most assessments for alcohol abuse, for example, ask about frequency of drink consumption. People from different countries tend to drink substances of different potencies and in different sizes. Effective measures must adapt the beverage referred to, the drink sizes assumed, and the amount of time asked about to be appropriate for the cultural background (WHO, 2000). For example, some assessments ask about drink usage in the past 7 days. These assessments would not be culturally appropriate for individuals from rural Mexico, who drink heavily only at seasonal fiestas (WHO, 2000).
Suggestions for professionals providing treatment for immigrants and refugees
Community professionals must be able to provide necessary services in as culturally responsible manner as possible. There are often limitations to providing such culturally tailored treatments (i.e., resources, training, money, etc.). When working with immigrants and refugees, it is important to focus on models that are inclusive of the family and systemic values (i.e., multiple causal factors, multidirectionality) because familial relationships promote protective factors for immigrants (Kim, Zane, & Hong, 2002). Different types of family-based treatments have been developed – some focusing on helping many families at one time, while others focus on individual families.
Group-based treatment. Group-based treatment can be helpful for immigrants because it provides a community context for healing. Social support is an essential part of behavior change (Mendenhall et al., 2012). Immigrants have often left behind important sources of social support (Pantin et al., 2003), which can be hard to duplicate in their new country. Effective treatments will rebuild some social support networks. Karen refugees, for example, report a direct connection between rebuilding communities and cultures that have been devastated by conflict, flight, displacement and resettlement and solving community-wide problems like substance use, intimate partner violence and stressed parent-child relationships. In focus groups, many Karen participants said that community rebuilding would be an essential part of recovery from harmful alcohol use (McCleary, 2013; McCleary & Wieling, in press).
Interventions that are group-based may involve the entire family or just specific members to experience the intervention. For example, an intervention may focus on the parents with the intent of participants implementing their new knowledge when they go back into their own family. Others may follow the protocols that include engaging the entire family in the intervention. Pantin et al. (2003) implemented a study to prevent substance use among immigrant adolescents which highlighted the needs of parents; the program included key variables of parenting, such as, communication, parenting behavioral problems, and parental involvement. These key variables seemed to be common in many interventions that focus on parents. For example, in a family treatment, Litrownik et al. (2000) focused on parent-child communication. Additional variables unique to this study included providing psychosocial information and social skills training. Marsiglia et al. (2010) similarly found familial communication to be helpful when working with adolescents of Mexican heritage. Adolescents were also taught decision making and risk assessment. Clearly adults and adolescents have some common needs (e.g., communication), but given their differing developmental levels (Carter & McGoldrick, 2005), it is appropriate that there be some differences in treatment also.
Family Therapy. Another route for intervention may be the treatment of the individual family. While this mode of treatment will be different depending on the provider and the family receiving services, there are some key components to keep in mind for treatment. Immigrant and refugee peoples may be in need of special consideration for potential differences in family structure and dynamics, religious considerations, language challenges, collectivism/individualism, hierarchy, gender roles, acculturation, and ethnic identity exploration (Rastogi & Wadhwa, 2006). Additionally, the provider must also focus on the identified problem the family wishes to address. Clearly this makes for complex needs and increases the need for clinicians to be culturally aware.
Culturally adapted programs
A small number of articles have described how they altered traditional substance abuse treatment programs to fit specific populations. Morelli, Fong, and Oliveira (2001) conducted a study on a residential, culturally competent substance abuse treatment for Asian/Pacific Islander mothers in Hawaii in which children could be with their mothers over the course of the program. The treatment program included traditional healing practices, infant healthcare services, and community elders lead the women in “infant-mother bonding” time. The women in the program found it especially helpful to, among other things, incorporate a blend of traditional healing practices along with conventional treatment methods, allowing mothers to be with their children in a nonjudgmental environment and working with “consistent and competent” staff members.
Another study illustrated how Alcoholics Anonymous (AA) was adapted to suit immigrants from Central America. Hoffman (1994) reported factors such as location of AA meetings, adapting treatment to fit subpopulations within the Latino/a community in Los Angeles and incorporating the traditional 12 steps with group-specific values. The location of these AA meetings was crucial in getting young Latinx males involved in the programs. Some meetings were held in churches, others in storefront buildings, and others in more traditional rental spaces. These decisions were carefully made to ensure the groups’ abilities to reach their targeted populations. Some groups utilized a theme of Machismo in Terapia Dura (Rough Therapy) to remind members of the negative impact alcohol can have on their lives. Some elements of Terapia Dura include aggressiveness and competitiveness. Groups varied in their use of Machismo based on levels of acculturation and group values. Though such groups were not culturally sensitive to women’s and homosexual members’ needs, they provided a way to treat a specific group of people who have previously been shown to do poorly in traditional AA groups.

Amodeo, Peou, Grigg-Saito, Berke, Pin-Riebe, and Jones (2004) described a culturally specific treatment for Cambodian immigrants. The study implemented culturally significant techniques such as utilizing acupuncture, providing therapy in the participants’ native language, incorporating Buddhist believes, consulting with an advisory board of members of the Cambodian community, emphasizing relationships, cultural values, and coping mechanisms, as well as doing home visits and utilizing culturally relevant data gathering questionnaires. This treatment approach also took into consideration the location services would be provided. They chose a location that was respected and well known in the Cambodian community.
33.8 End-of-Chapter Summary
As previously stated, the topic of substance abuse prevalence and treatment within immigrant and refugee communities is complex as it involves many different types of populations representing different cultures, resources, traditions, and challenges. For some populations, family connection has been found to be a protective factor against substance abuse, but there is simply an overall dearth of research on the topic. It is clear that more research is needed across each of the areas discussed in this chapter specific to immigrant and refugee communities: theoretical, policy, familial, methodological and intervention-based. Additionally, it has been several years since the United States has published a comprehensive study on prevalence rates for substance abuse among immigrants and refugees (Brown et al., 2005). Given how much our country has changed politically, economically, and demographically in the past decade, it may be timely for the National Surveys on Drug Use and Health to publish the prevalence rates within the more recent 2013 survey and for other researchers to focus on substance use among immigrant and refugee populations.
Case Study
Jon is a 23-year-old first-generation Laotian man who has been using heroin for the past two years. Recently, he has been evaluated and recommended to attend drug treatment. Jon’s parents struggle to understand what addiction is. Historically, Jon’s father has struggled with alcohol abuse; his family reframes his drinking as normal behavior.
Prior to his heroin use, Jon used marijuana exclusively. Fifteen years ago, John came with his family (i.e., parents, younger brother, and older sister) from Vietnam as a refugee.
Jon states that he must return to work in order to help his family pay for living expenses (i.e., rent, food, transportation, medication). The family also supports extended family members back home in Vietnam; these family members are dependent on these financial remittances. Jon agrees that he needs to change, but struggles knowing how to make changes and with his motivation to change.
Jon appears to use the fact that he is proficient in English to his advantage. When communicating with employees at the treatment facility and with court representatives, he communicates different information to different staff members. He also continues this pattern with his family members. Jon does this by leaving out important details for his family and not translating his parents’ express wishes for his discharge. Jon states that his family does not understand addiction and therefore, do not need to be involved in his discharge recommendation planning.
- How might the living situation of newly immigrated refugees influence Jon’s substance use and treatment?
- Can you list 2-3 services in your community that would address Jon and his family needs on different subsystems? Would these resources be culturally sensitive and appropriate?
- What are some common intervention strategies that may encourage Jon’s family to engage in his treatment?
- How has traumatic stress potentially contributed to Jon’s substance abuse? How do you believe traumatic stress has impacted other generations of Jon’s family?
- What are some cultural barriers Jon faces in seeking treatment?
Helpful Links
Drug and Alcohol Use in Refugee Communities
- https://practicetransformation.umn.edu/webinars/drug-and-alcohol-use-in-refugee-communities/
- This webinar by Dr. Simmelink McCleary describes how immigrants and refugees understand substance use and trauma, with guidelines for treatment providers.
References
Akinsulure-Smith, A. M. & O’Hara, M. (2012). Working with forced migrants: Therapeutic issues and considerations for mental health counselors. Journal of Mental Health Counseling, 34, 38-55.
Almeida, J., Johnson, R. M., Matsumoto, A., & Godette, D. (2012). Substance use, generation and time in the United States: The modifying role of gender for immigrant urban adolescents. Social Science & Medicine, 75(12), 2069–2075. http://doi.org/10.1016/j.socscimed.2012.05.016.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders: DSM-5. Washington, D.C: American Psychiatric Association.
Amodeo, M., Peou, S., Grigg-Saito, D, Berke, H., Pin-Riebe, S., & Jones, L. K. (2004). Providing culturally specific substance abuse services in refugee and immigrant communities: Lessons from a Cambodian treatment and demonstration project. Journal of Social Work Practice in Addictions, 4(2) 23-46.
Arfken, C. L., Berry, A., & Owens, D. (2009). Pathways for Arab Americans to substance abuse treatment in southeastern Michigan. Journal of Muslim Mental Health, 4(1), 31-46. doi: 10.1080/15564900902785457.
Bacio, G. A., Mays, V. M., & Lau, A. S. (2012). Drinking initiation and problematic drinking among Latino adolescents: Expectations of the immigrant paradox. Psychology of Addictive Behaviors, October, 1-9.
Barnes, D. M., Harrison, C., & Heneghan, R. (2004). Health Risk and Promotion Behaviors in Refugee Populations. Journal of Health Care for the Poor and Underserved, 15(3), 347-356.
Baumrind, D. (1971). Current patterns of parental authority. Developmental Psychology, 4, 1-103. http://psycnet.apa.org/doi/10.1037/h0030372.
Betancourt, T. S., Abdi, S., Ito, B. S., Lilienthal, G. M., Agalab, N., & Ellis, H. (2015). We left one war and came to another: Resource loss, acculturative stress, and caregiver–child relationships in Somali refugee families. Cultural Diversity and Ethnic Minority Psychology, 21(1), 114-125. http://dx.doi.org.ezp2.lib.umn.edu/10.1037/a0037538.
Betancourt, T. S., Newnham, E. A., Layne, C. M., Kim, S., Steinberg, A. M., Ellis, H., & Birman, D. (2012), Trauma History and Psychopathology in War-Affected Refugee Children Referred for Trauma-Related Mental Health Services in the United States. Journal of Traumatic Stress, 25, 682–690. doi: 10.1002/jts.21749.
Birman, D., & Tran, N. (2008). Psychological distress and adjustment of Vietnamese refugees in the United States: Association with pre- and post-migration factors. American Journal of Orthopsychiatry, 78(1), 109-120.
Boss, P. (1991). Ambiguous loss. In Walsh, F., & McGoldrick, M. (Eds.), Living beyond loss: Death in the family. W.W. Norton & Company: New York, NY.
Breslau, J., & Chang, D.F. (2006). Psychiatric disorders among foreign-born and us-born Asian Americans in a us national survey. Social Psychiatry and Psychiatric Epidemiology, 41(12), 943-950.
Bronfenbrenner, U. (1977). Toward the experimental ecology of human development. American Psychologist, July, 513-531.
Brown, J. M., Council, C. L., Penne, M. A., & Gfroerer, J. C. (2005). Immigrants and substance use: Findings from the 1999–2001 National Surveys on Drug Use and Health (DHHS Publication No. SMA 04–3909, Analytic Series A-23). Rockville, MD: Substance Abuse and Mental Health Services Administration, Office of Applied Studies.
Carter, B., & McGoldrick, M. (2005). The expanded family life cycle: Individual, family, and social perspectives (3rd Ed.). New York, NY: Allyn & Bacon.
Centers for Disease Control and Prevention. (2015). Excessive drinking costs U.S. $223.5 billion. Retrieved from http://www.cdc.gov/features/alcoholconsumption/.
Chartier, K. G., & Caetano, R. (2011). Trends in alcohol services utilization from 1991–1992 to 2001–2002: ethnic group differences in the US population. Alcoholism: Clinical and Experimental Research, 35(8), 1485-1497.
Cook, W. K., Bond, J., Karriker-Jaffe, K., J., & Zemore, S (2013). Who’s at risk? Ethnic drinking cultures, foreign nativity, and problem drinking among Asian American young adults. Journal of Studies on Alcohol and Drugs, 74(4), 532-541.
D’Avanzo, C.E. (1997). Southeast Asians: Asian-Pacific Americans at risk for substance misuse. Substance Use & Misuse, 32(7-8), 829-848. doi: 10.3109/10826089709055861.
Dillon, F. R., de la Rosa, M., Sanchez, M., & Schwartz, S. J. (2012). Preimmigration family cohesion and drug/alcohol abuse among recent Latino immigrants. The Family Journal, 20(3) 256-266.
Driscoll, A. K., Russell, S. T., & Crockett, L. J. (2008). Parenting styles and youth well-being across immigrant generations. Journal of Family Issues, 29, 185-209.
Engel, G. L. (1977). The need for a new medical model: A challenge for biomedicine. Science, 196(4286), 129-136. doi: 10.1126/science.847460.
Escobar, J. I., Nervi, C.H., & Gara, M.A. (2000). Immigration and mental health: Mexican Americans in the united states. Harvard Review of Psychiatry, 8(2), 64-72.
Ezard, N. (2012). Substance use among populations displaced by conflict: A literature review. Disasters, 36(3), 533-557. doi: 10.1111/j.1467-7717.2011.01261.x
Ezard, N., Oppenheimer, E., Burton, A., Schilperoord, M., Macdonald, D., Adelekan, M., &Van Ommeren, M. (2011). Six rapid assessments of alcohol and other substance use in populations displaced by conflict. Conflict and Health, 5(1). doi: 10.1186/1752-1505-5-1.
Farrell, A.D., & White, K.S. (1998). Peer influences and drug use among urban adolescents: Family structure and parent-adolescent relationship as protective factors. Journal of Consulting and Clinical Psychology, 66(2), 248-258. http://psycnet.apa.org/doi/10.1037/0022-006X.66.2.248.
Gee, G. C., Delva, J., & Takeuchi, D. T. (2007). Relationships between self-reported unfair treatment and prescription medication use, illicit drug use, and alcohol dependence among Filipino Americans. American Journal of Public Health, 97(5), 933-940.
Gwyn, P. G., & Colin, J. M. (2010). Research with the doubly vulnerable population of individuals who abuse alcohol. Journal of Psychosocial Nursing, 48(2) 38-43.
Hernandez, D. J., Denton, N. A., Macartney, S., & Blanchard, V. L. (2012). Children in immigrant families: Demography, policy, and evidence for the immigrant paradox. In C.G. Coll & A.K. Marks (Eds.), The immigrant paradox in children and adolescents: Is becoming American a developmental risk? (pp. 17-36). Washington, DC: American Psychological Association.
Hoffman, F. (1994). Cultural adaptations of alcoholics anonymous to serve Hispanic populations. International Journal of Addictions, 29(4), 445-460. doi: 10.3109/10826089409047392.
Hussey, J. M., Hallfors, D. D., Waller, M. W., Iritani, B. J., Halpern, C. T., & Bauer, D. J. (2007), Sexual behavior and drug use among Asian and Latino adolescent: Association with immigrant status. Journal of Immigrant Health, 9, 85-94.
Iguchi, M.Y., Bell, J., Ramchand, R.N., & Fain, T. (2005). How criminal system racial disparities may translate into health disparities. Journal of Health Care for the Poor and Underserved, 16(4), 48-56. doi: 10.1353/hpu.2005.0114.
Institute of Medicine. (2002). Unequal Treatment: What healthcare providers need to know about racial and ethnic disparities in health care. Retrieved from: https://www.nap.edu/catalog/10260/unequal-treatment-confronting-racial-and-ethnic-disparities-in-health-care
Jamil, H., Hakim-Larson, J., Farrag, M., Kafaji, T., Jamil, L. (2002). A retrospective study of Arab American mental health clients: Trauma and the Iraqi refugees. American Journal of Orothpsychatry, 72(3), 355-361.
Jensen, S. B. (1996). Mental health under war conditions during the 1991–1995 war in the former Yugoslavia. World Health Statistics Quarterly, 49, 213–217.
Johnson, H., & Thompson, A. (2008). The development and maintenance of post-traumatic stress disorder (PTSD) in civilian adult survivors of war trauma and torture: A review. Clinical Psychology Review, 28(1). 36-47. http://dx.doi.org/10.1016/j.cpr.2007.01.017.
Kam, J. A. (2011). The effects of language brokering frequency and feelings on Mexican-heritage youth’s mental health and risky behaviors. Journal of Communication, 61, 455-475.
Kandula, N. R., Kersey, M., & Lurie, N. (2004). Assuring the health of immigrants: What the leading health indicators tell us. Annual Reviews of Public Health, 25, 357-376.
Kim, I. J., Zane, N. W., & Hong, S. (2002). Protective factors against substance use among Asian American youth: A test of the peer cluster theory. Journal of Community Psychology, 30(5), 565-584.
Kulis, S., Marsiglia, F. F., Sicotte, D., & Nieri, T. (2007). Neighborhood effects on youth substance us in a southwestern city. Sociological Perspectives, 50(2) 273-301.
Letzter-Pouw, S. E., Shrira, A., Ben-Ezra, M., & Palgi, Y. (2014). Trauma transmission through perceived parental burden among Holocaust survivors’ offspring and grandchildren. Psychological Trauma: Theory, Research, Practice, and Policy, 6(4), 420-429. doi:10.1037/a0033741.
Litrownik, A. J., Elder, J. P., Campbell, N. R., Ayala, G. X., Slymen, D. J., Parra-Medina, D., Zavala, F. B., & Lovato, C. Y. (2000). Evaluation of a tobacco and alcohol use prevention program for Hispanic migrant adolescents: Promoting the protective factor of parent-child communication. Preventative Medicine, 31, 124-133.
Luitel, N. P., Jordans, M., Murphy, A., Roberts, B., & McCambridge, J. (2013). Prevalence and patterns of hazardous and harmful alcohol consumption assessed using the AUDIT among Bhutanese refugees in Nepal. Alcohol and Alcoholism, 48(3), 349-355. http://dx.doi.org/10.1093/alcalc/agt009.
Marlatt, G. A. (1992). Substance abuse: Implications of a biopsychosocial model for prevention, treatment, and relapse prevention. In J. Grabowski & G.R. VandenBos (Eds.), Psychopharmacology: Basic Mechanisms and Applied Interventions (pp. 131-162). Washington, DC: American Psychological Association.
Marshall, G. N., Schell, T. L., Elliott, M. N., Berthold, S., & Chun, C. (2005). Mental Health of Cambodian Refugees 2 Decades After Resettlement in the United States. JAMA, 294(5):571-579. doi:10.1001/jama.294.5.571.
Marsiglia, F. F., Kulis, S., Parsai, M., Villar, P., & Garcia, C. (2009). Cohesion and conflict: family influences on adolescent alcohol use in immigrant Latino families. Journal of Ethnicity in Substance Abuse, 8, 400-412.
Marsiglia, F. F., Kulis, S., Yabiku, S. T., Nieri, T. A., & Coleman, E. (2010). When to intervene: Elementary school, middle school or both? Effects of keepin’ it REAL on Substance use trajectories of Mexican heritage youth. Prevention Science, 12, 48-62.
Mautino, K. S. (2002). Immigrants, immigration, and substance use and abuse. Journal of Immigrant Health, 4(1) 1-3.
McCleary, J. S. (2013). An exploration of alcohol use in Karen refugee communities in the context of conflict-related displacement. Unpublished doctoral dissertation. University of Minnesota.
McClearly, J. S., & Wieling, E. (in press). Forced displacement and alcohol use in two Karen refugee communities: A comparative qualitative study. The British Journal of Social Work.
Mena, M. P., Mitrani, V. B., Muir, J. A., & Santisteban, D. A. (2008). Extended parent-child separations: Impact on substance-abusing Hispanic adolescents. Journal for Specialists in Pediatric Nursing, 13(1) 50-52.
Mendenhall, T. J., Seal, K.L., GreenCrow, B. A., LittleWalker, K. N., & BrownOwl, S. A. (2012). The family education diabetes series: Improving health in an urban-dwelling American Indian community. Qualitative Health Research, 22, 1524-1534.
Morelli, P. T., Fong, R., & Oliveira, J. (2001). Culturally competent substance abuse treatment for asian/pacific islander women. Journal of Human Behavior in the Social Environment, 3(3-4), 263-280. doi: 10.1300/J137v03n03_16.
Moya, E. M., & Shedlin, M. G. (2009). Policies and laws affecting Mexican-origin immigrant access and utilization of substance abuse treatment: Obstacles to recovery and immigrant health. Substance Use & Misuse, 43(12-13), 1747-1769. doi: 10.1080/10826080802297294.
National Drug Intelligence Center (NDIC). (2011). National drug threat assessment. Retrieved from https://www.justice.gov/archive/ndic/pubs44/44849/44849p.pdf
Organista, K. C. (2007). Towards a structural-environmental model of risk for HIV and problem drinking in Latino labor migrants: the case of day laborers. Journal of Ethnic & Cultural Diversity in Social Work, 16(1-2), 95-125.
Palmer, R. H. C., Brick, L., Nugent, N. R., Bidwell, L. C., McGeary, J. E., Knopik, V. S., & Keller, M. C. (2015). Examining the role of common genetic variants on alcohol, tobacco, cannabis and illicit drug dependence: genetics of vulnerability to drug dependence. Addiction, 110(3), 530-537. doi: 10.1111/add.12815.
Pantin, H., Schwartz, S. J., Sullivan, S., Coatsworth, J. D., & Szapocznik, J. (2003). Preventing substance abuse in Hispanic immigrant adolescents: An ecodevelopmental, parent-centered approach. Hispanic Journal of Behavioral Sciences, 25, 469-500.
Porter, M., & Haslam, N. (2005). Predisplacement and postdisplacement factors associated with mental health of refugees and internally displaced persons. The Journal of the American Medical Association, 294(5), 602-612. doi: 10.1001/jama.294.5.602.
Prado, G., Huang, S., Schwartz, S. J., Maldonado-Molina, M. M., Bandiera, F. C., de la Rosa, M., & Pantin, H. (2009). What accounts for differences in substance use among U.S.-born and immigrant Hispanic adolescents? Results from a longitudinal prospective cohort study. Journal of Adolescent Health, 45, 118-125.
Pumariega, A. J., Millsaps, U., Rodriguez, L., Moser, M., & Pumariega, J. B. (2007). Substance abuse in immigrant Latino youth in Appalachia. Addictive Disorders & Their Treatment, 6(4) 157-165.
Rastogi, M., & Wadhwa, S. (2006). Substance abuse among Asian Indians in the United States: A consideration of cultural factors in etiology and treatment. Substance Use & Misuse, 41, 1239-1249.
Rebhun, L. A. (1998). Substance use among immigrants to the united states. In S. Loue (Ed.), Handbook of Immigrant Health (pp. 493-519). New York, NY: Springer US.
Roberts, S., & Nuru-Jeter, A. (2012). Universal screening for alcohol and drug disparities in child protective services reporting. Journal of Behavioral Health Services & Research, 39(1) 3-16.
Salas-Wright, C. P., Vaughn, M. G., Clark, T. T., Terzis, L. D., & Cordova, D. (2014). Substance use disorders among first- and second-generation immigrant adults in the United States: evidence of an immigrant paradox? Journal of Studies on Alcohol and Drugs, 75(6), 958-987.
Schwartz, S. J., Mason, C. A., Pantin, H., & Szapocznik, J. (2008). Effects of family functioning and identity confusion on substance use and sexual behavior in Hispanic immigrant early adolescents. Identity: An International Journal of Theory and Research, 8(2), 107-124.
Sotero, M. (2006). A conceptual model of historical trauma: Implications for public health practice and research. Journal of Health Disparities Research and Practice, 1(1), 93-108.
Streel, E., & Schilperoord, M. (2010). Perspectives on alcohol and substance abuse in refugee settings: Lessons from the Field. Intervention, 8(3) 268-275.
Szaflarski, M., Cubbins, L.A., & Ying, J. (2011). Epidemiology of alcohol abuse among us immigrant populations. Journal of Immigrant and Minority Health, 13(4), 647-658. doi: 10.1007/s10903-010-9394-9.
Szapocznik, J. & Coatsworth, J. D. (1999). An ecodevelopmental framework for organizing the influences on drug abuse: A developmental model of risk and protection. In Glantz, M. D. & Hartel, C. R. (Eds). Drug abuse: Origins & Interventions. American Psychological Association: Washington D. C.
United Nations. (2014). Global trends 2013. Geneva, Switzerland: Author.
United States Department of Health and Human Services (USDHHS). (2014). The health consequences of smoking—50 years of progress: A report from the Surgeon General. Retrieved from: http://www.surgeongeneral.gov/library/reports/50-years-of-progress/full-report.pdf
Weaver, H., & Roberts, B. (2010). Drinking and displacement: A systematic review of the influence of forced displacement on harmful alcohol use. Substance Use & Misuse, 45(13), 2340-2355. doi: 10.3109/10826081003793920.
World Health Organization. (2000). International guide for monitoring alcohol consumption and related harm. Retrieved from: http://apps.who.int/iris/bitstream/10665/66529/1/WHO_MSD_MSB_00.4.pdf.
Attribution
Adapted from Chapters 1 through 9 from Immigrant and Refugee Families, 2nd Ed. by Jaime Ballard, Elizabeth Wieling, Catherine Solheim, and Lekie Dwanyen under the Creative Commons Attribution-NonCommercial 4.0 International License, except where otherwise noted.
